
What is the Iliotibial Band Syndrome?
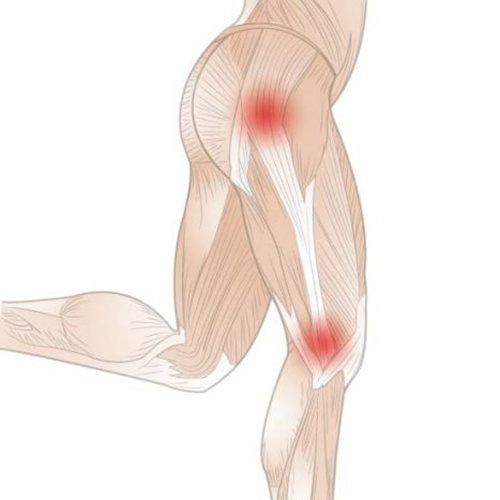
The iliotibial band is a thick band of connective tissue that runs from the hip bone and outer thigh down to the lateral tibial plateau on the shin. Iliotibial band syndrome (ITBS) is a common overuse injury in which the iliotibial band becomes irritated around the outside of the knee after repeated loading. During knee flexion, the iliotibial band moves over the lateral femoral epicondyle, and the tissue beneath it can become irritated.
You need your iliotibial band to stabilise the knee joint during running and repetitive bending activities. So, if the iliotibial band becomes irritated or overloaded, movement becomes painful. If the problem is severe, you may not be able to run, hike downhill, cycle hard, or train in the gym comfortably for weeks or even months.
You may also see the term ‘iliotibial band friction syndrome’. This misnomer reflects an older explanation that the iliotibial band ‘rubs’ over the bone at the lateral femoral epicondyle. Current thinking often describes the problem as compression and irritation of the tissue beneath the iliotibial band during repetitive bending and knee flexion, rather than friction.
What is the Iliotibial Band Syndrome?
The iliotibial band is a thick band of connective tissue that runs from the hip bone and outer thigh down to the lateral tibial plateau on the shin. Iliotibial band syndrome (ITBS) is a common overuse injury in which the iliotibial band becomes irritated around the outside of the knee after repeated loading. During knee flexion, the iliotibial band moves over the lateral femoral epicondyle, and the tissue beneath it can become irritated.
You need your iliotibial band to stabilise the knee joint during running and repetitive bending activities. So, if the iliotibial band becomes irritated or overloaded, movement becomes painful. If the problem is severe, you may not be able to run, hike downhill, cycle hard, or train in the gym comfortably for weeks or even months.
You may also see the term ‘iliotibial band friction syndrome’. This misnomer reflects an older explanation that the iliotibial band ‘rubs’ over the bone at the lateral femoral epicondyle. Current thinking often describes the problem as compression and irritation of the tissue beneath the iliotibial band during repetitive bending and knee flexion, rather than friction.

Iliotibial Band Syndrome Symptoms
Iliotibial band syndrome symptoms usually feel like knee pain and pain on the outside of your knee that starts during an activity and gets worse the longer you keep going. Many people confuse ITBS with a knee injury because the main symptom is lateral knee pain and swelling. Pain on the outside of your knee can be sharp pain or a dull ache. Iliotibial band syndrome swelling is not always obvious, but some people notice mild puffiness or tenderness at the outer knee, especially after a flare-up.
You can often identify the problem as originating from the iliotibial band if you bend your knee to about 45 degrees and feel pain on the outside of your knee.
Symptoms are commonly worse when you run on uneven or downhill terrain, hike downhill, climb stairs repeatedly, cycle with heavy gearing, or train with repeated squats and lunges during a flare-up.
Some also report iliotibial band syndrome hip pain, usually as aching or tightness around the outer hip, because the iliotibial band connects to hip muscles that help control the leg. Hip abductor weakness can allow the knee to drift inward, causing hip pain.
Risk factors include excessive foot pronation, poor running posture, internal tibial torsion, muscle tightness, and sudden increases in load, especially in distance runners. Your podiatrist can identify which risk factors apply to you.
When to See a Podiatrist for ITBS
You should see a podiatrist when running with iliotibial band syndrome stops you from activities, keeps returning, or does not improve after two to three weeks of smart load changes. ITBS requires early assessment, as treatment early in the cycle can lead to better outcomes than if left untreated.
If you have significant symptoms, such as severe pain at rest or at night, significant or increasing swelling, a locked knee, giving way, a recent twist injury, or very focal pain over the bone, book an appointment soon. These features may point to other conditions that can mimic ITBS.

Diagnosis of Iliotibial Band Syndrome
To diagnose iliotibial band syndrome, our podiatrist at The Foot Practice uses a careful history and physical examination, with imaging mainly used to rule out other problems in the affected leg or legs. Swelling and tenderness can be felt along the iliotibial band. Our podiatrist will often ask about recent load changes, downhill exposure, cambered routes, shoe changes, cycling setup changes, or new gym programmes. Your clinician may also use provocation tests that load the outer knee and assess hip strength and control.
Conservative treatment with physical therapy and mobilisation exercises is key. Gait and footwear assessment are important as ITBS is not only about knee pain. The way your foot loads and how your leg rotates can influence knee control during stance. At The Foot Practice, we may use RehaWalk® pressure-sensor treadmill gait analysis to measure stride length, cadence, step width and pressure patterns that may be contributing to recurrent flare-ups.
X-rays and imaging tests are only done to rule out another problem with the knee. Magnetic resonance imaging (MRI) can be performed if the diagnosis is in doubt and may show soft-tissue thickening in the iliotibial band, changes in the lateral synovial recess, or adjacent tissue changes at the lateral femoral epicondyle. These results may change management strategies.

Iliotibial Band Syndrome Treatment
Iliotibial band syndrome treatment usually involves conservative, non-surgical management that helps reduce irritation, improve strength, and guide a gradual return to activity.. The best way to treat ITBS is to stop provoking activities or reduce your overall activity load as soon as you feel the pain causing pain to worsen. This will become a chronic problem if you keep going at the same intensity.
Instead of running, do cross-training by swimming, rowing, cycling, and water-resistance running in the pool, as long as these do not trigger symptoms. Pain medicines can help with short-term pain control, and many people use an ice pack on the outer knee after activity. It is also helpful to know that heat may feel soothing, but it can aggravate irritability for some people if used too early.
Avoid aggressive foam-roller work and deep pressure on the outside of the knee. Some feel temporarily better after using a foam roller, but the pain may flare up again quickly. Manual therapy, back, and musculoskeletal rehabilitation may help.

A reliable plan focuses on three pillars:
- Settle the flare-up without losing fitness: The goal is to reduce the specific load that causes pain while maintaining aerobic capacity and lower-limb function. Many people do well with level walking, cycling in lighter gears, or modified gym work that does not reproduce symptoms.
- Build strength where it matters: ITBS often improves when you build hip strength and endurance, particularly the hip abductor muscles that control side-to-side stability, and when you restore calf, biceps femoris and trunk capacity that supports efficient movement. A physical therapist can guide strengthening exercises that start with basic hip control work and progress to heavier strength work, such as split squats and step-down variations, once you can go downstairs without pain. Strength work should progress until it matches the demands of your goals, not just until pain settles.
- Adjust mechanics and load progression: Small changes can help reduce stress while you rebuild capacity. For some runners, slightly increasing cadence or adjusting foot strike can reduce overstriding. For cyclists, adjusting saddle height or cleat position may reduce knee stress. For gym training, reducing depth, volume, or load in squats and lunges can help early on.
Footwear, Orthoses and The Foot Practice Approach
ITBS can flare up because of worn-out shoes with poor midsole support, inconsistent stability across your shoe rotation, or a sudden change in training surface. A footwear assessment helps identify whether your shoes suit your mechanics and activity demands.
Orthoses can help certain people if excessive foot pronation or foot loading patterns contribute to repeated strain and pain. The goal is not to ‘fix pronation’ but to support more repeatable loading and reduce compensations during longer sessions.
RehaWalk® gait analysis can help map whether you are offloading one side, whether pressure shifts are increasing strain, and whether changes in cadence or step width are likely to help. It also gives objective markers to track progress.
Iliotibial Band Syndrome Injection
If symptoms do not improve with conservative care, your podiatrist may discuss a local corticosteroid injection, which can reduce pain in the short term. They work best paired with rehabilitation and should be used sparingly and thoughtfully by your healthcare provider.
Surgical Options for Iliotibial Band Syndrome
Surgical options exist, but if none of the above measures work, surgery can be performed to release part of the iliotibial band or address the repeatedly irritated tissue. If surgery is being considered, you will usually be referred to an orthopaedic specialist.
Risks and Recovery Time
Iliotibial band syndrome recovery time depends on how long you have had symptoms, how reactive the pain is, and how closely your load progression matches your capacity. In many, ITBS symptoms improve over a few weeks with smart modifications and consistent strength work. For others, especially if ITBS has become persistent, recovery can take longer.
A practical way to think about the healing time for iliotibial band syndrome is that pain on the outside of your knee can settle before capacity returns. If you resume full training as soon as pain subsides, recurrence is common. Building strength and endurance usually takes longer than settling the initial flare.
The main risks are recurrence from repeating the same load errors, loss of fitness and capacity due to excessive rest, and missing a different diagnosis if the pain does not fit typical ITBS patterns. For example, medial compartment arthritis can be confused with ITBS.
How to Prevent Iliotibial Band Syndrome
How to prevent iliotibial band syndrome comes down to training progression, surface choices, strength capacity, and shoe consistency.
Rest the leg or reduce load on days when pain on the outside is most severe. Before harder sessions, warm up and build intensity gradually.
Check your footwear for wear and support. If there is a wear pattern that suggests instability, replace your shoes before they contribute to repeat flare-ups. Avoid sudden spikes in downhill work and be cautious with banked surfaces. If you run on a circular track, change direction regularly to reduce repeated loading on the same side.
Try not to do all your training on very hard surfaces if you get predictable symptom flares. Keep a base of hip and lower-limb strengthening as part of your weekly routine, even after your symptoms settle. For many, that is the most effective long-term prevention tool.

How The Foot Practice Can Help
If iliotibial band syndrome is limiting your sport, work, or day-to-day activity, you do not need to guess your way through it. The Foot Practice in Singapore can assess your symptoms, review your footwear and load triggers, and, where appropriate, use gait tools such as RehaWalk® and 3D infrared gait analysis to guide a clear, staged plan. We focus on settling the flare-up, restoring capacity, and reducing recurrence so you can return to the activities you value. Make an appointment at our sports podiatry clinic today.





